

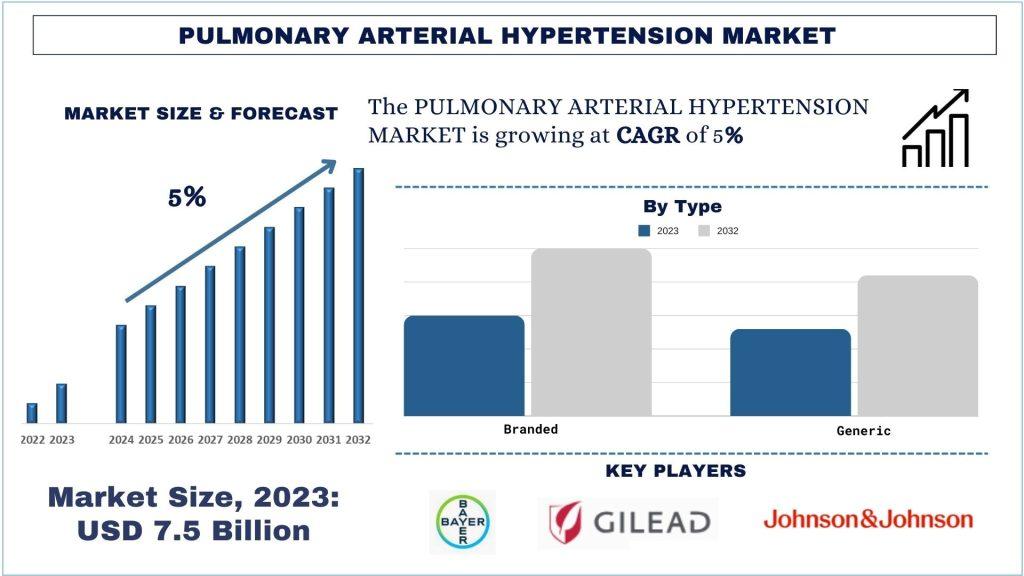
According to a new report by Univdatos Market Insights, the Pulmonary Arterial Hypertension Market is expected to reach USD 11.5 Billion in 2032 by growing at a CAGR of ~5%. The uncommon and progressive condition known as pulmonary arterial hypertension (PAH) is typified by elevated blood pressure in the pulmonary arteries, which transport blood from the heart to the lungs. These arteries narrow and stiffen as a result of this disorder, increasing blood flow resistance and placing additional load on the right side of the heart. Over time, significant problems such as right heart failure may arise from PAH. Breathlessness, exhaustion, dizziness, chest pain, and swelling in the legs and ankles are common symptoms. Idiopathic, heritable, or linked to other conditions such chronic liver illness, congenital heart disease, or connective tissue abnormalities are some possible diagnoses for PAH.
Access sample report (including graphs, charts, and figures): https://univdatos.com/get-a-free-sample-form-php/?product_id=61552
Over recent years, the incidence and prevalence of PAH have been steadily rising globally. This trend is attributed to factors such as changes in lifestyle, dietary habits, environmental factors, and improved diagnostic techniques leading to better detection rates. The growing patient pool is a significant driver for the expansion of the PAH market. For instance, as per the data of American Heart Association (AHA) 2021, the prevalence of PAH in the United States is estimated to be between 15 and 50 cases per million people, with an incidence of about 2-5 cases per million adults annually.
Therapeutic Landscape of Pulmonary Arterial Hypertension
1. Endothelin Receptor Antagonists (ERAs):
Endothelin receptor antagonists are a cornerstone of PAH therapy. These drugs work by blocking the effects of endothelin-1, a potent vasoconstrictor that contributes to the narrowing of pulmonary arteries. Common ERAs include:
· Bosentan (Tracleer): An oral dual endothelin receptor antagonist that improves exercise capacity and slows disease progression.
· Ambrisentan (Letairis): A selective ERA that targets the endothelin A receptor, leading to vasodilation and reduced pulmonary artery pressure.
· Macitentan (Opsumit): A dual ERA with a longer half-life, providing sustained effects in reducing PAH symptoms and progression.
2. Phosphodiesterase-5 Inhibitors (PDE-5i):
Phosphodiesterase-5 inhibitors enhance the effects of nitric oxide, a vasodilator, by preventing its breakdown. This leads to relaxation of pulmonary arteries and improved blood flow. Key PDE-5 inhibitors used in PAH treatment include:
· Sildenafil (Revatio): Initially developed for erectile dysfunction, sildenafil is effective in improving exercise capacity and hemodynamics in PAH patients.
· Tadalafil (Adcirca): Another PDE-5 inhibitor that offers a longer duration of action, providing once-daily dosing for PAH management.
3. Prostacyclin Analogs and Prostacyclin Receptor Agonists:
Prostacyclin analogs and receptor agonists mimic the effects of prostacyclin, a natural vasodilator that inhibits platelet aggregation and smooth muscle proliferation. These therapies are particularly beneficial for patients with advanced PAH:
· Epoprostenol (Flolan, Veletri): An intravenous prostacyclin analog that has shown significant benefits in survival and symptom relief.
· Treprostinil (Remodulin, Tyvaso, Orenitram): Available in intravenous, subcutaneous, inhaled, and oral formulations, treprostinil offers flexible administration options.
· Iloprost (Ventavis): An inhaled prostacyclin analog used for its ease of administration and targeted pulmonary effects.
· Selexipag (Uptravi): An oral prostacyclin receptor agonist that provides prostacyclin-like effects with convenient dosing.
4. Soluble Guanylate Cyclase (sGC) Stimulators:
· sGC stimulators enhance the nitric oxide signaling pathway, leading to vasodilation and improved blood flow in the pulmonary arteries:
· Riociguat (Adempas): The first approved sGC stimulator for PAH, riociguat improves exercise capacity and delays clinical worsening.
5. Calcium Channel Blockers (CCBs):
Calcium channel blockers are used in a subset of PAH patients who respond positively to acute vasoreactivity testing. These medications help relax the blood vessels and reduce pulmonary artery pressure:
Nifedipine and Diltiazem: Commonly used CCBs for patients with a positive vasoreactivity test.
6. Combination Therapy:
Combination therapy involves using two or more PAH medications with different mechanisms of action to achieve better control of symptoms and disease progression. This approach has become increasingly common as research shows improved outcomes compared to monotherapy. For example, combining an ERA with a PDE-5 inhibitor or a prostacyclin analog can provide synergistic benefits.
Click here to view the Report Description & TOC - https://univdatos.com/report/pulmonary-arterial-hypertension-market/
Conclusion
In conclusion, the treatment landscape for PAH is diverse and continuously evolving. The development of targeted therapies, combination regimens, and emerging treatments offers hope for improved management and outcomes for PAH patients. Continued research and innovation are essential to further advance the field and provide new options for those affected by this challenging condition.
Related Healthcare Market Research Report
Colorectal Cancer Market: Current Analysis and Forecast (2024-2032)
Polymer-Based Prefilled Syringe Market: Current Analysis and Forecast (2024-2032)
Pipette Tips Market: Current Analysis and Forecast (2024-2032)
Dental Connected Technology Solutions Market: Current Analysis and Forecast (2024-2032)
Contact Us:
UnivDatos Market Insights
Email - contact@univdatos.com
Contact Number - +1 9782263411
Website - https://univdatos.com/
Linkedin- https://www.linkedin.com/company/univ-datos-market-insight/mycompany/